
Cardiovascular Risk Assessment

Cardiovascular diseases such as ischemic heart disease, thrombosis, arterial hypertension with its complications – myocardial infarction and stroke – constitute a dynamic multistep process that is closely related to inflammation1. It is well-known that CVD diseases rank first among all other diseases of mankind. Traditionally for making an accurate diagnosis, the patient must undergo a series of procedures, undergo lab tests so that the doctor can prescribe the necessary treatment. However, there is another way. Doctors and individuals sometimes use general heart-health checklists to stay aware of wellness indicators. This time, not only will we consider different methods / risk calculators that are now used in clinical practice, but we’ll illustrate how lifestyle-oriented risk quizzes work with a hypothetical scenario. And, of course, let’s talk about why, given the presence of such intelligent systems, the CVD problem is still relevant.
This article was last reviewed by Svetlana Baloban, Healsens, on January 24, 2020. This article was last modified on December 15, 2020.
Why do you need cardiovascular risk assessments?
Before proceeding to describe various calculation methods, let’s find out why they are needed at all. To begin with, we shall that most heart diseases develop completely asymptomatically over many years. In practice, it means that if one doesn’t feel any health problems, he or she simply does not go to the doctor unless a critical condition occurs. So, according to some estimates, 3.7 million Americans2 remain with undiagnosed heart disease. At the same time, the highest proportion of undiagnosed CVDs, which led to death from cardiovascular diseases, is among people aged 18–59 years. This is especially true when you consider that obesity, type 2 diabetes, and other risk factors are becoming more common at a young age.
Second, recognizing general risk factors can encourage healthier habits and discussions with a healthcare professional. And thirdly, the assessment of risk factors can clearly demonstrate how the total risk changes if you switch to a healthier lifestyle.
That is why, as early as in 1948, the Framingham Heart Study was initiated under the direction of the US National Heart, Lung, and Blood Institute. It was an ambitious medical research project that changed the medicine we know.
As part of this study, the main risk factors for cardiovascular disease were identified. These include the following indicators:
- high blood cholesterol
- high blood pressure
- smoking
- obesity
- diabetes
- lack of physical activity.
IN THIS ARTICLE
RELATED ARTICLES
Valuable information has also been obtained on the role of cholesterol, age, gender, and psychological problems. During this time, the risk assessment has changed and developed significantly. In this article, we will analyze what cardiovascular risk assessment means and what calculators are used now in medical practice.
Follow us on Facebook|| Instagram || Telegram || Youtube
SCORE Risk Chart (Systematic Coronary Risk Evaluation)
The European guidelines for cardiovascular disease (CVD) prevention recommend the use of modified SCORE risk charts. SCORE highlights long-term lifestyle trends linked to overall heart health so readers can see how changes in habits might influence their well-being3.
The first Joint Working Group of European societies on coronary prevention used a simple risk chart. For their calculations, they considered the following categories:
- age;
- gender;
- smoking status;
- assessment of total cholesterol;
- assessment of systolic blood pressure.
Then, the diagram became more complex in order to assess risks more accurately. So, in addition to total cholesterol, the ratio of cholesterol to HDL cholesterol was also taken into account in risk assessments.
Why Healsens?
Healsens — a holistic approach to healthy living with wellness tracking and general tips—all in one place.
🔗 Explore Healsens on Google Play / App Store for general wellness tracking.
In addition, given the geographic variability in cardiovascular risk across Europe, two SCORE charts have been developed for countries with high and low CVD risk. Countries with low risk include countries such as Andorra, Austria, Belgium, Cyprus, Denmark, Finland, France, Germany, Greece, Iceland, Ireland, Israel, Italy, Luxembourg, Malta, Monaco, Netherlands, Norway, Portugal, San Marino , Slovenia, Spain, Sweden, Switzerland and the United Kingdom of Great Britain and Northern Ireland.
Countries at high risk of CVD: Bosnia and Herzegovina, Croatia, Czech Republic, Estonia, Hungary, Lithuania, Montenegro, Morocco, Poland, Romania, Serbia, Slovakia, Tunisia and Turkey.
And the group of countries with a very high risk (note that the diagrams may underestimate the risk in these countries) included such countries as: Albania, Algeria, Armenia, Azerbaijan, Belarus, Bulgaria, Egypt, Georgia, Kazakhstan, Kyrgyzstan, Latvia, North Macedonia , Moldova, Russian Federation, Syrian Arab Republic, Tajikistan, Turkmenistan, Ukraine and Uzbekistan.
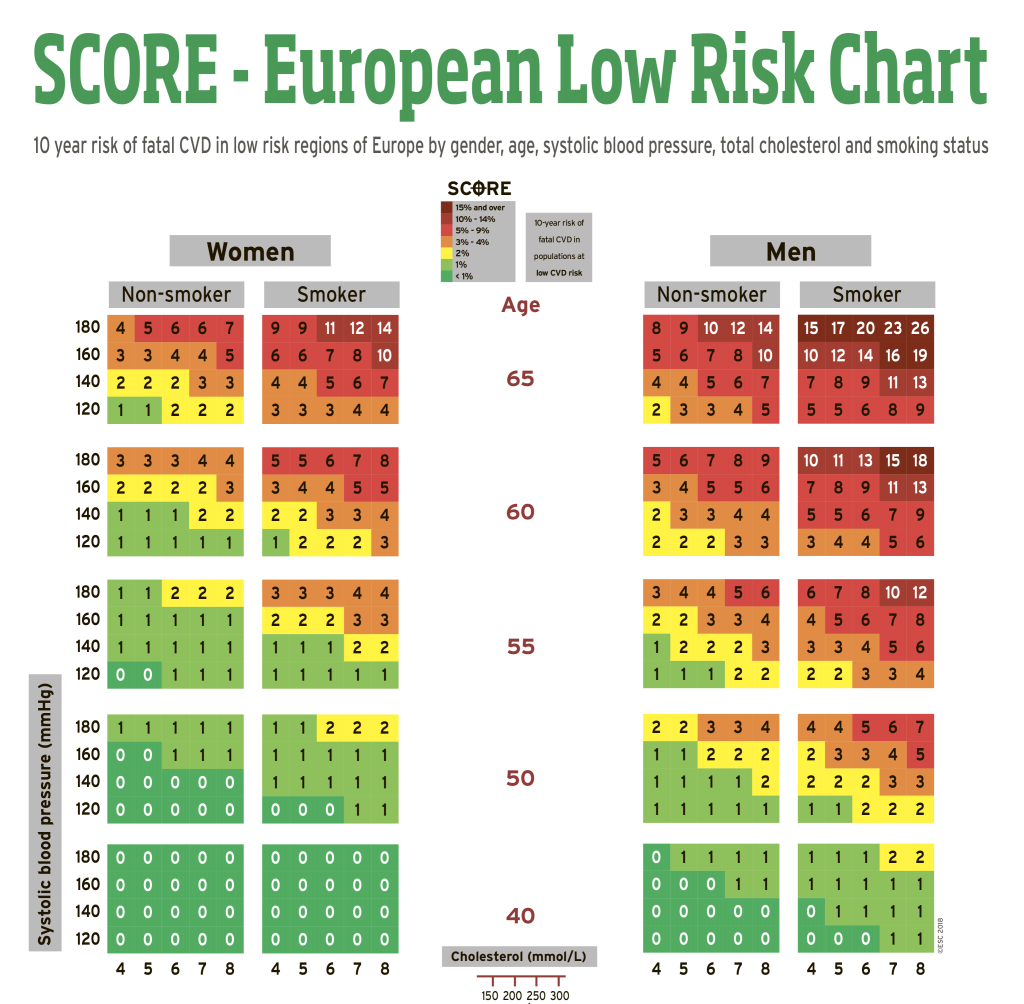
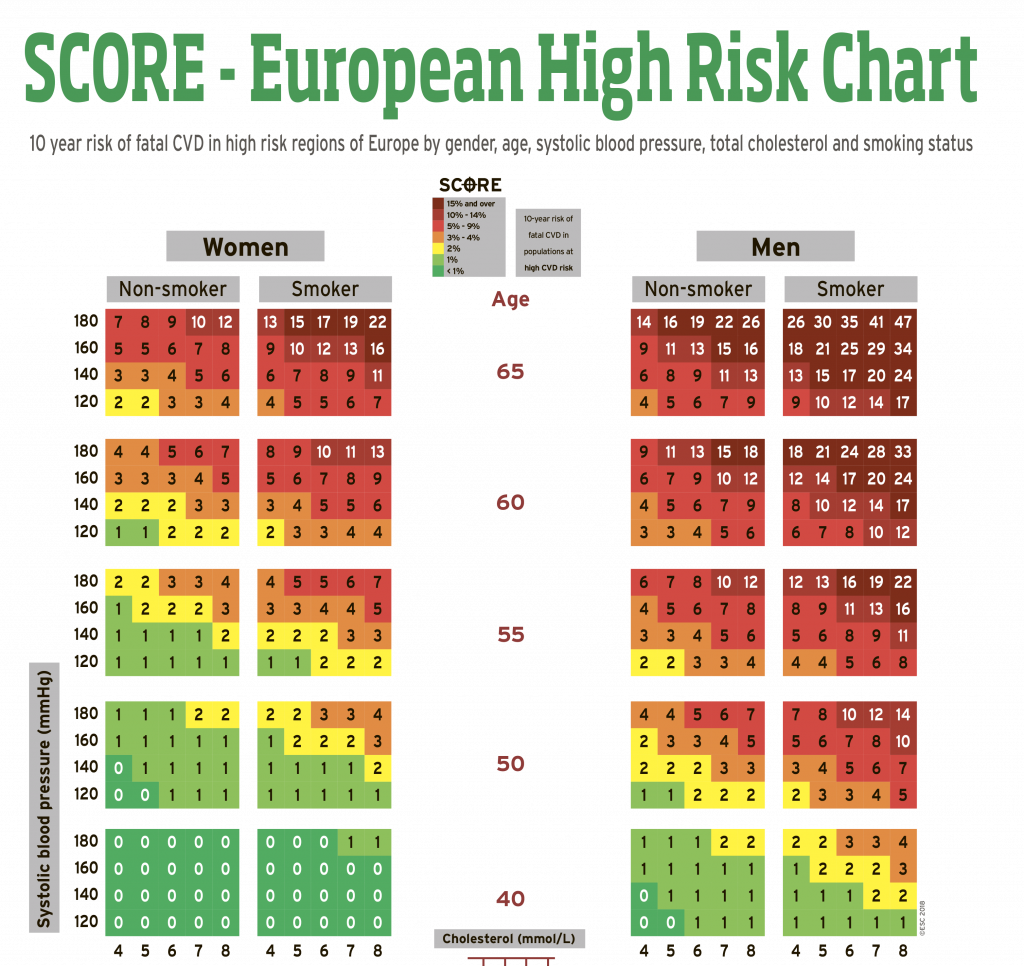
Based on the data reflected on it, one can conclude about the level of risk:
- high risk (above 10%) in the presence of two or more risk factors;
- moderately high (5-10%) in the presence of two or more risk factors;
- moderate risk (1–5%) in the presence of two or more risk factors;
- low risk (below 1%) in the absence of risk factors or the presence of only one.
Due to this SCORE scale, the following cardiovascular diseases can be detected: stroke, myocardial infarction, pulmonary embolism, dissecting aortic aneurysm.
» Wondering why you should calculate your biological age? These 5 reasons will convince you to do it now.
Framingham Risk Score
The Framingham scale provides a snapshot of lifestyle-related factors that clinicians use to spark conversations about staying heart-healthy over the next decade. Like the SCORE scale, this system opens the door for making a forecast for the next 10 years. This scale was developed in North America. Thus, NCEP 4 recommends the Framingham Risk Score for cardiovascular risk assessment. You can also calculate it by yourself.
The total risk on the Framingham scale is defined as:
- low (risk below 10%);
- medium (risk from 10 to 20%);
- high (risk above 20%).
A value over 30% indicates a very high risk of cardiovascular disease.
A 10-year risk estimate can be obtained as a percentage, which is then used to make decisions about disease prevention. This assessment is also evolving. For example, in 2009 CCS added additional risks to the Framingham risk scale4. It included a family history of coronary heart disease in a first-line relative. It takes into account male first-degree relative younger than 55 years and female first-degree relative younger than 65 years old. For elderly patients, sensitive C-reactive protein results can also help to reclassify risks.
Reynolds Risk Score
If you are healthy and do not have diabetes, Reynolds Risk Score gives people a sense of how their current habits compare to clinical benchmarks so they can prioritize heart-healthy behaviors. The risk calculation is designed for people aged 45 and over. The scale assesses the following risk factors: gender, age, systolic blood pressure, total and “good” (high-density lipoprotein) cholesterol, hs C-reactive protein level, myocardial infarction in parents under 60 years of age, smoking. You can calculate it yourself on the website http://www.reynoldsriskscore.org/.
For the Reynolds scale, a risk score of 10-15% is considered a moderate risk of cardiovascular disease over the next five years.
If the risk estimate is less than 10%, then the patient is considered to be at low risk of cardiovascular disease for the next five years.
» Discover everything about what your cholesterol results mean.
ASCVD (Atherosclerotic Cardiovascular Disease) Risk Score
The Atherosclerotic Cardiovascular Disease Risk Scale (ASCVD) is a national guideline developed by the American College of Cardiology. ASCVD-style estimates offer a broad picture of how lifestyle choices relate to heart health, which may help people prepare for more informed discussions with their doctor. This risk calculator is considered an important step forward in assessing the risk of both heart disease and stroke and provides estimates that are applicable to Blacks / African Americans. It is used among patients with no pre-existing cardiovascular disease aged 40 to 79 years.
The calculator has also been tested against the final USPSTF guidelines for initiating aspirin therapy5. It is also included in the JNC-8 guidelines for blood pressure management6.
The ASCVD percentage is used by clinicians; if you’re curious about heart wellness, discuss any results with your doctor before considering medications.
PROCAM Score (Prospective Cardiovascular Munster Study)
PROCAM-style scoring highlights how current habits align with clinical patterns, giving users context for maintaining long-term heart wellness.
This wellness quiz looks at common heart-health factors and offers general risk categories to discuss with your clinician.
QRISK (QRESEARCH Cardiovascular Risk Algorithm)
QRISK-style outputs illustrate how age, activity, and other lifestyle factors trend with cardiovascular health, helping people stay mindful of areas they can improve.
Assessing factors of the QRISK scale: age, gender, smoking, body mass index, family predisposition to cardiovascular diseases, treatment with drugs that reduce high blood pressure. The age for assessing QRISK ranges from 25 to 84 years old. Low risk – QRISK2 score less than 10%. This means that the likelihood of a stroke or heart attack in the next 10 years is less than one in ten. Moderate risk – QRISK2 10-20%. High risk – QRISK2 score over 20%. This means that a person has at least two out of ten chances of having a heart attack in the next 10 years.
Moreover, when a patient is admitted to a hospital, the GRACE scale can also be used; clinicians use separate hospital tools for complex cases; Healsens focuses on everyday wellness awareness.
Follow us on Facebook|| Instagram || Telegram || Youtube
The 65yo Patient’s CVD Risks
As an example, let’s review the case of a patient who was admitted to the intensive care unit 3 hours before dying of myocardial infarction at the age of 65. His complaints include vomiting, nausea, weakness, and shortness of breath that appeared within an hour of admission to the emergency department. On the eve of the event, the patient several times consulted the doctor about pain in the stomach and uncontrolled vomiting. The main risks include smoking with more than 40 years of experience. The man did not have diabetes or hypertension.
| Cholesterol | 6.43 | mmol / L |
| Cholesterol – HDL | 1.02 | mmol / L |
| Cholesterol – LDL | 4.56 | mmol / L |
| Triglycerides | 1.32 | mmol / L |
| C-reactive protein | 3 | mg / L |
| Blood pressure | 120/80 | Hg |
Using sample numbers, various heart-health scores show how results can differ; only a clinician can interpret them for care.
- ASCVD score – 20.8% (high risk)
- SCORE scale – 12.7% (high risk)
- Framingham risk – 18.6% (average risk)
- according to Reynolds – 19% (high risk)
- by the PROCAM scale – 60 points or> 40% (high risk)
- result on the QRISK risk scale – 23.5% (high risk)
- on the ASSIGN scale – 30 (high risk)
In this example, no follow-up lifestyle support was provided despite elevated wellness risk indicators.
Effectiveness of Using CVD Risk Scoring
So, the main factors in the development of CVD are known and there are effective and safe methods of treatment, however, cardiovascular diseases remain the main cause of death and severe disability worldwide. What’s the matter?
The problem is that traditional methods of preventing cardiovascular disease have proven to be insufficient. First, in practice, only 60-65% of cardiovascular diseases are identified using risk calculations7. In addition, the data showed that calculated risks do not always lead to disease development. Conversely, many acute clinical events occur in patients with moderate or no risk. This is most likely due to the fact that many other factors are not included in such calculations. The problem is also that there is no single risk assessment system. Therefore, different organizations offer their own options.
Finally, absolute risk based guidelines for cardiovascular disease (CVD) prevention are poorly used worldwide8! Although the guidelines available, the absolute risk is often not assessed. And even when it is assessed, it is not necessarily used to make management decisions as we see in the above case of a 65-year-old patient.
Finally, we add that studies have unequivocally shown that different CVD risk scales are the best signal for a patient showing it is time to change lifestyle in order to reduce risk factors9. These wellness calculators can raise awareness; Healsens offers similar score estimates to help users discuss lifestyle steps with their doctor10. To download the application, follow the links below.
FURTHER READING
Source: ©️2019 Healsens B.V. All right reserved
Follow us on Facebook|| Instagram || Telegram || Twitter || Youtube
Source: ©️2019 Healsens B.V. All right reserve
- Inflammation – Cause or Consequence of Heart Failure or Both?
- Undiagnosed Heart Conditions
- SCORE Risk Charts
- 009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult – 2009 recommendations
- Aspirin Use to Prevent Cardiovascular Disease and Colorectal Cancer: Preventive Medication
- 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults
- Assessment and Relevance of Carotid Intima-Media Thickness (C-IMT) in Primary and Secondary Cardiovascular Prevention
- Implementing cardiovascular disease prevention guidelines to translate evidence-based medicine and shared decision making into general practice: theory-based intervention development, qualitative piloting and quantitative feasibility
- Should heart age calculators be used alongside absolute cardiovascular disease risk assessment?
- Effect of using cardiovascular risk scoring in routine risk assessment in primary prevention of cardiovascular disease: an overview of systematic reviews

