From Tracking to Transformation: How Doctors Use Wearable Data in Clinical Practice
From Tracking to Transformation: How Doctors Use Wearable Data in Clinical Practice Read More »

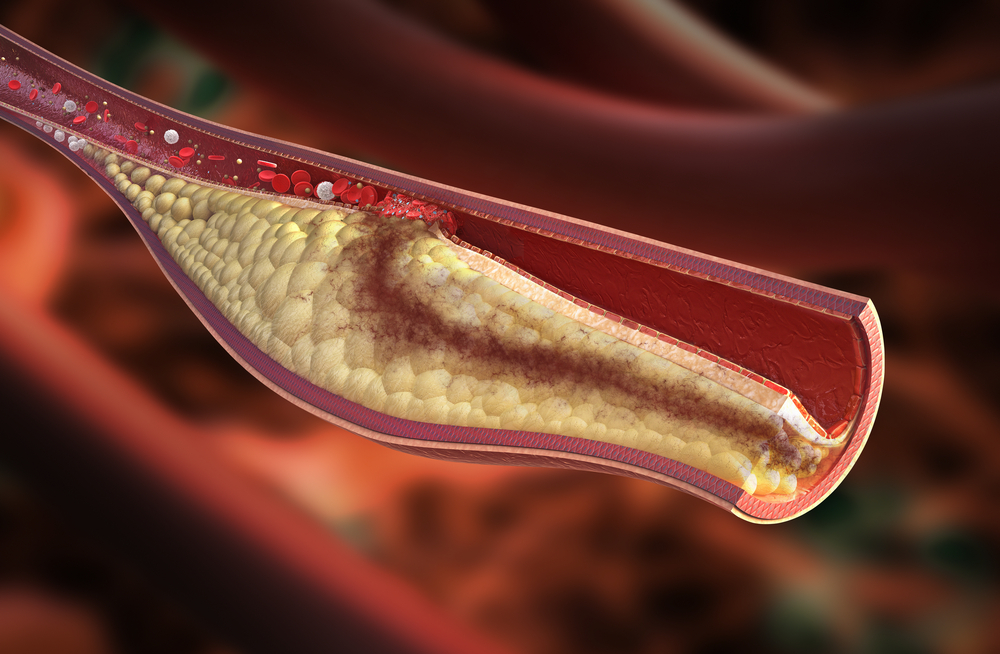
Keeping your heart healthy is something you can work on every day.
What you eat, how much you move, whether you smoke and controlling your cholesterol and blood pressure are five things that can have a big impact on your heart.